
Frozen Shoulder Study Case
R2P <> Oro Muscles INTRO – Case Summary
This case involved a 26–27 year old female patient, a graphic designer, not an athlete.
She had a history of recurrent shoulder dislocations and eventually underwent surgery. After surgery, she started physiotherapy in two different clinics. The rehab was too aggressive early on, which led to significant muscle guarding and eventually a frozen shoulder.
By the time she came to me, she had been dealing with this for about four months. She had already seen two clinics before and had started to lose confidence — not only in physiotherapy, but also in herself and her ability to recover.
Pain was preventing her from lifting her arm properly. Her main goal was simple: she just wanted to return to normal daily life activities like showering, reaching overhead, or grabbing objects from shelves. She wasn’t trying to return to sport, she just wanted her shoulder back.
Her chief complaint was that she could not actively abduct her shoulder without shrugging. She was always compensating with excessive upper trapezius activation and lateral trunk flexion. Even when looking in a mirror, she couldn’t correct it.
THE CHALLENGE
The main challenge was motor control.
Even though we improved her passive range of motion with manual therapy, dry needling, and mobility work, she still couldn’t actively abduct properly. She wanted to perform the movement correctly, but her body kept choosing the wrong strategy.
It wasn’t a strength issue anymore — it was a motor pattern issue. She would automatically recruit upper trap instead of her middle deltoid, starting from around 45° to 60° of abduction.
Before using Oro, my hypothesis was that the deltoid was under-activating and the upper trap was overcompensating, but I couldn’t objectively show her that.
Traditional assessment showed limited active control and poor movement quality, but I couldn’t quantify the compensation pattern.
WHY I USED ORO
I decided to use Oro almost spontaneously. She told me that even at the gym, her trainer noticed she was always shrugging during lateral raises. So I thought — let’s measure it.
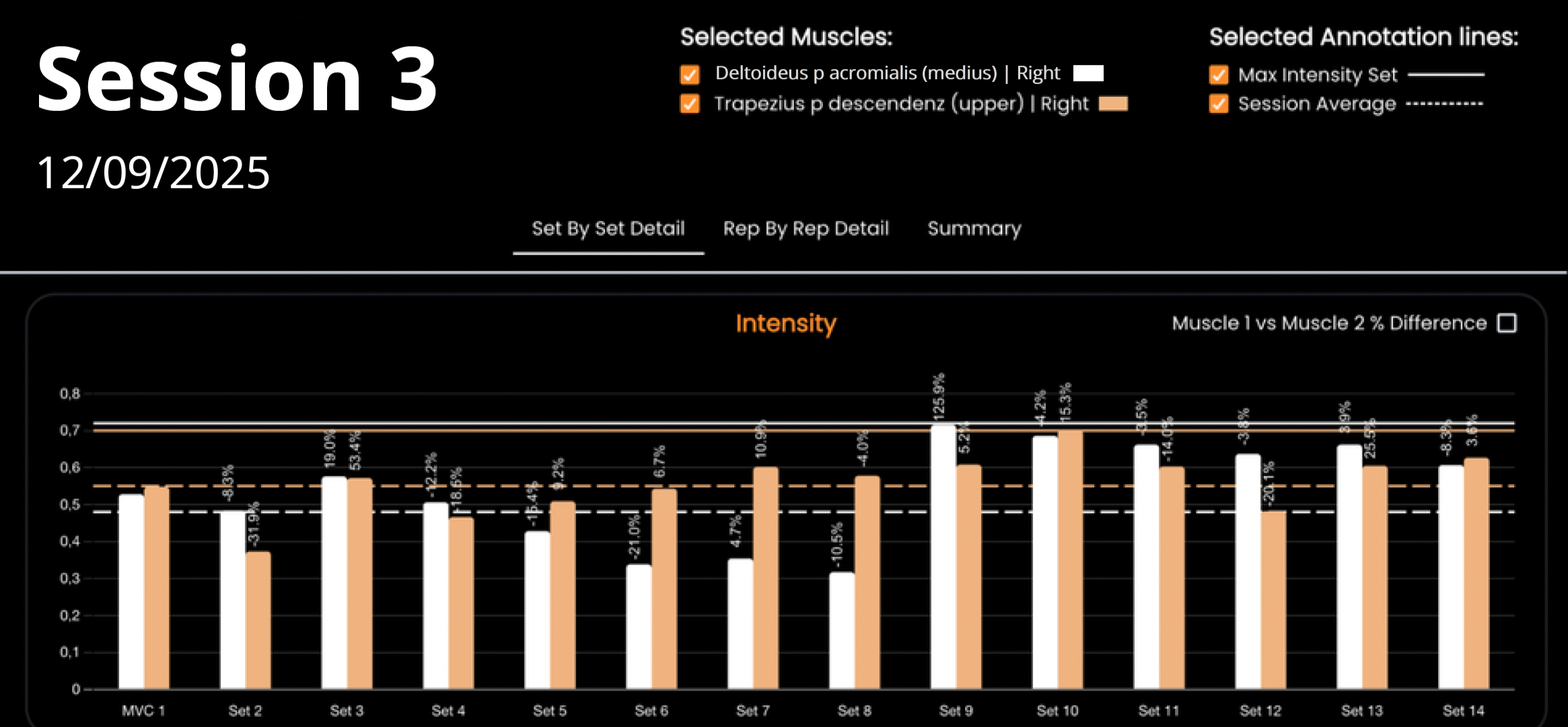
I placed one electrode on the middle deltoid and one on the upper trapezius.
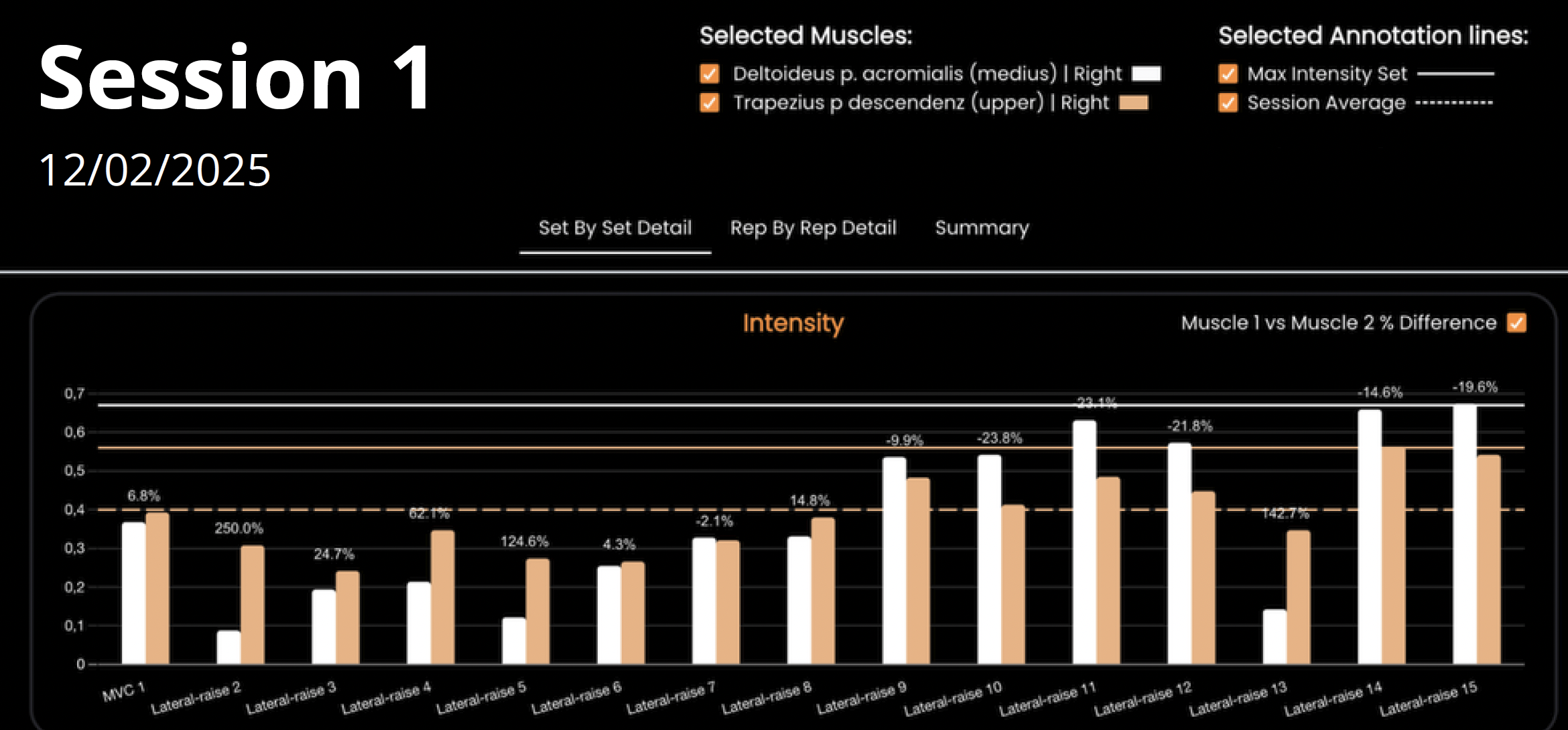
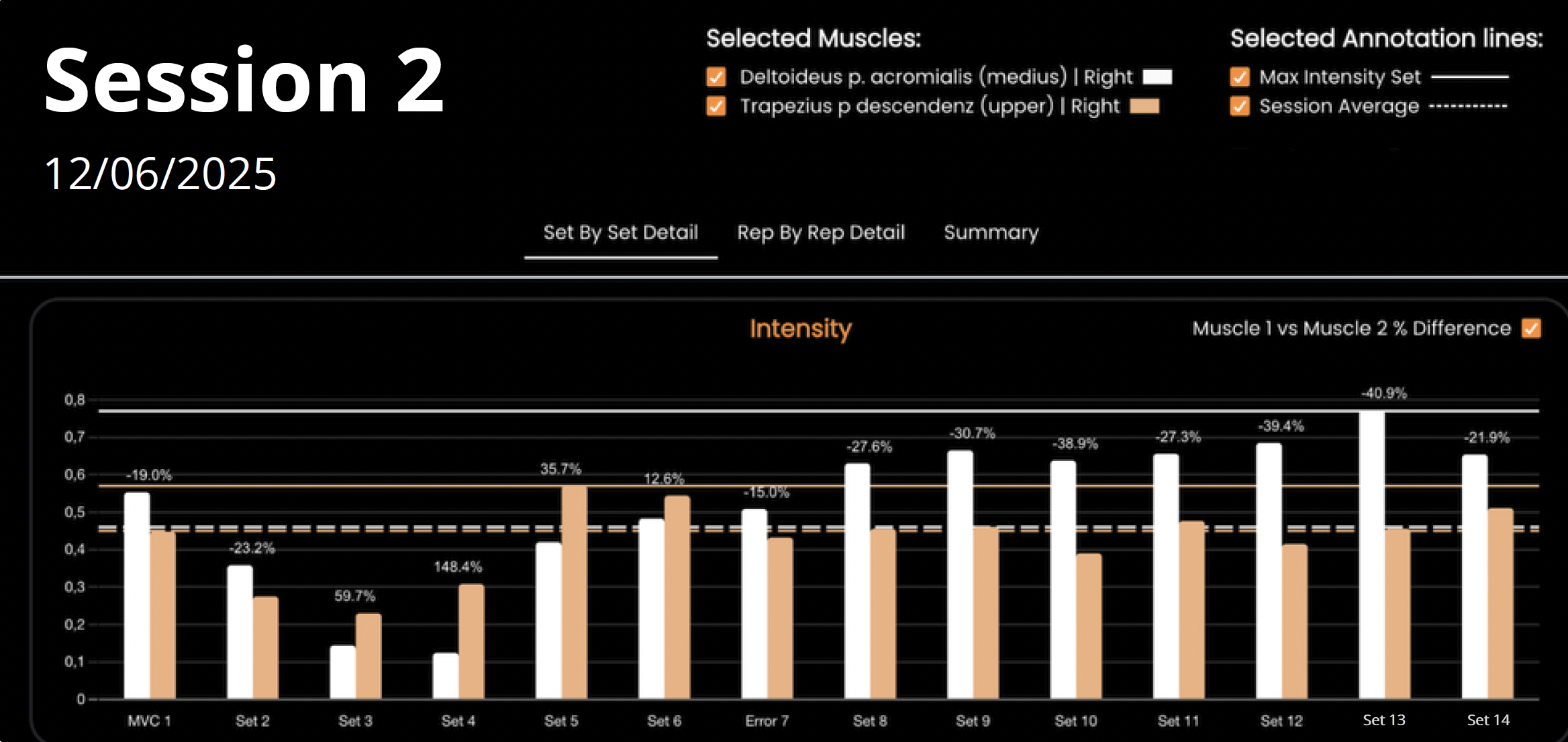
We started with isometric abduction around 60° during the first session, because that was approximately where compensation appeared. From the second session onward, we progressed to dynamic movements.
First, we performed the movement without resistance. Then I applied manual resistance carefully — just enough to challenge the deltoid without forcing upper trap dominance.
What Oro revealed was very clear. At baseline, the deltoid activation was low and the trap was dominating. With visual biofeedback, when I told her, “inflate the orange ball without inflating the blue ball,” she immediately improved.
TREATMENT PLAN & IMPLEMENTATION
Oro didn’t replace my treatment plan — it enhanced it.
We were already working on mobility and soft tissue restrictions. Oro allowed us to directly target the motor control deficit.
We used real-time biofeedback for motor learning. She performed repetitions until fatigue. When she said she was tired, I could see the deltoid activation dropping on the screen, which validated the neuromuscular fatigue.
The most impressive part was retention. After practicing with the screen, I asked her to repeat the movement without looking. She was able not only to maintain the correct activation pattern, but to sustain it over time in subsequent sessions.
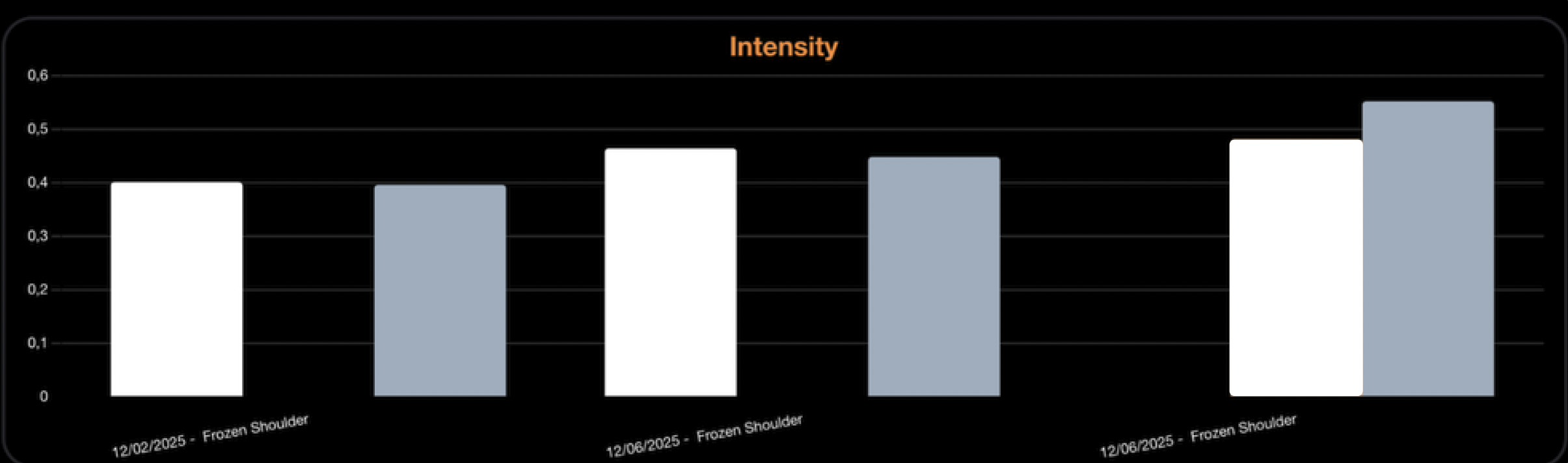
We used Oro across three sessions total.
Session one at the end of treatment.
Sessions two and three at the beginning of treatment to reinforce motor learning.
After that, the goal was achieved and we moved on.
GOALS & OUTCOMES
My goal was to restore clean active abduction without compensation, eliminate pain, and rebuild her confidence.
In similar cases without EMG feedback, correcting this type of compensation usually takes two to three weeks.
In her case, the activation issue was corrected within minutes.
Objectively, we saw improved deltoid activation, reduced trap dominance, better movement quality, improved endurance over repetitions, and full active abduction without compensation.
Subjectively, she reported no more pain when lifting her arm, no more shrugging compensation, and significantly more confidence.
An important point is that she had already seen several physiotherapists before. Experiencing such a rapid and visible improvement restored her trust — both in the rehabilitation process and in herself. That psychological shift was just as important as the physical improvement.
CLINICAL INSIGHTS & LEARNINGS
What surprised me most was how fast it worked.
Before this case, I thought Oro would require dedicating a large portion of the session. Instead, it took only a few minutes and integrated seamlessly into normal practice.
It also reinforced the importance of early implementation. If we had used this earlier in her rehab, we might have prevented the chronic compensation pattern from settling in.
Since then, I’ve started thinking more about early neuromuscular activation assessment in similar cases.
I actually have another patient coming in who reports upper trap fatigue during lateral raises despite no ROM limitation. I will use the same approach.
So yes, I would absolutely use Oro again for similar motor control deficits. And beyond shoulder cases, I see value anywhere movement quality and muscle recruitment patterns matter, especially in early-stage rehab.
WRAP-UP
The key takeaway for me is that sometimes the problem is not mobility or strength, but motor strategy. And when patients can see their activation in real time, it changes everything.

Get in touch!
Our team is here to make your journey seamless! If you have questions, you can directly get in contact: